
The topic of radiation therapy for spinal and bone marrow tumors is clinically significant for two principal reasons. First, spinal involvement represents one of the most common patterns of skeletal metastasis and is associated with severe pain, pathological fractures, neurological deficits, and loss of mobility. Second, bone marrow simultaneously serves as a therapeutic target (in certain hematologic malignancies and in conditioning regimens prior to hematopoietic stem cell transplantation) and as a critical organ highly sensitive to ionizing radiation. This dual role limits the possibilities for dose escalation and necessitates a carefully balanced integration of radiation therapy with systemic treatment modalities.
From an epidemiological perspective, Russian clinical guidelines on metastatic bone disease emphasize that skeletal-related events include pathological fractures and spinal cord compression; metastases to the axial skeleton (including the spine) are particularly frequent, and osteolytic lesions in multiple myeloma are observed in the vast majority of patients [1, 2]. The goals of radiation therapy in spinal and bone marrow tumors are pragmatic: rapid and durable pain relief; prevention and treatment of spinal cord compression; achievement of local control (especially in oligometastatic disease or radioresistant histologies); postoperative consolidation of high-risk areas; and, in selected primary tumors (e.g., chordomas), serving as a component of radical treatment with delivery of high radiation doses while maximally sparing the spinal cord. In general oncology practice, approximately half of all patients receive radiation therapy during the course of their disease, and its contribution to cure remains substantial, indirectly explaining the central role of this modality in the management of spinal lesions. An additional important aspect is the interdisciplinary decision-making at the interface of radiation oncology and neurosurgery. Contemporary treatment algorithms—most notably the NOMS framework—require assessment of neurological status and the degree of epidural extension, tumor radiosensitivity, mechanical spinal stability, and the patient’s systemic prognosis. Based on these factors, a decision is made between conventional radiation therapy, stereotactic radiation therapy, or surgical intervention (including decompression and stabilization) [3].
Physical Principles of Radiation Therapy in the Context of the Spine and Bone Marrow
Radiation therapy is based on the use of ionizing radiation to transfer energy to tissues; the key physical outcome is ionization and excitation of molecules, primarily water and biomacromolecules, which initiates a cascade of DNA damage. In clinical practice, megavoltage photon radiation therapy predominates. As photons pass through tissues in this energy range, the principal interaction mechanism is Compton scattering, which determines dose distribution in soft tissues, whereas the photoelectric effect plays a leading role at lower energies and in diagnostic imaging. These principles are fundamental for understanding dose deposition in the spinal cord and bone marrow: photon beams inevitably generate both entrance and exit doses along the beam path. In the anatomical region of the spine, dose-distribution physics acquires particular importance because the target (vertebral body or epidural tumor component) is often located only a few millimeters from the spinal cord. The clinical value of a technology is therefore determined by its ability to produce a steep dose gradient and to reproducibly ensure geometric accuracy of radiation delivery (immobilization, image guidance, and accounting for respiratory and postural micromovements). This explains the technological evolution from three-dimensional conformal radiation therapy (3D-CRT) to IMRT/VMAT and IGRT, and subsequently to SBRT/SRS in carefully selected clinical situations [4]. Proton and ion therapy differ physically from photon therapy: the maximum energy release occurs near the end of the particle range (the Bragg peak), theoretically allowing dose reduction beyond the target volume. For spinal tumors, this is particularly relevant when high focal doses must be delivered while minimizing the “dose tail” toward the spinal cord and other organs at risk. However, clinical implementation of proton therapy requires consideration of range uncertainties, tissue heterogeneity, and issues related to relative biological effectiveness (RBE). Contemporary reviews of innovations in radiation oncology emphasize that the development of proton and ion therapy, adaptive RT, and advanced dose-distribution strategies is aimed at improving the therapeutic index—escalating tumor dose while reducing exposure to normal tissues [5].
Radiobiological Features
The biological target of radiation therapy is cellular DNA. Double-strand breaks (DSBs) are considered the most critical type of damage, as they are strongly associated with loss of reproductive capacity and radiation-induced cell death. DNA damage occurs both through direct interaction of ionizing radiation with the DNA molecule and indirectly via free-radical reactions generated during water radiolysis. The latter mechanism is particularly significant in photon radiation therapy within the water-rich cellular environment. Cell death following irradiation may occur through various pathways (apoptosis, mitotic catastrophe, senescence, among others), and the clinical response is often delayed, developing over weeks after treatment completion [1]. The classical radiobiological rationale for fractionation is described by the concept of the four R’s: repair of sublethal damage, repopulation, redistribution within the cell cycle, and reoxygenation. These principles are directly reflected in the treatment of spinal metastases and bone marrow tumors. The choice between single-fraction regimens (e.g., 8 Gy) and multifraction schedules represents a clinical compromise between rapid palliation, safety for normal tissues, and the possibility of re-irradiation in cases of progression [2]. The spinal cord is the critical organ at risk in spinal irradiation. According to QUANTEC estimates, irradiation of the full cross-sectional area of the spinal cord to a cumulative dose of approximately 50 Gy with conventional fractionation is associated with a very low risk of radiation-induced myelopathy, whereas further dose escalation significantly increases complication probability [6]. For SBRT/SRS regimens, separate tolerance guidelines have been developed. Within the HyTEC recommendations for the spinal cord, estimated maximum dose (Dmax) constraints corresponding to approximately 1–5% risk of radiation myelopathy are reported as follows: about 12–14 Gy in 1 fraction, 17 Gy in 2 fractions, 20.3 Gy in 3 fractions, 23 Gy in 4 fractions, and 25.3 Gy in 5 fractions (with appropriate volume definition and reporting methodology) [7].
A practical implication is that, under borderline anatomical conditions, adherence to spinal cord constraints takes priority over full target coverage during inverse SBRT planning. Bone marrow tissue is highly radiosensitive due to the substantial proportion of actively proliferating cells. Clinical guidelines for multiple myeloma emphasize that local RT is typically delivered at relatively low total doses (approximately 10–30 Gy) or as a single 8 Gy fraction; dose escalation to 30–50 Gy does not improve clinical outcomes but may result in prolonged myelosuppression and hinder continuation of systemic therapy. Contemporary publications also highlight the risk of bone marrow fibrosis and cytopenias with inappropriate dosing, reinforcing the trend toward “low-but-effective-dose” palliative regimens in patients with multiple myeloma and plasmacytomas [8].
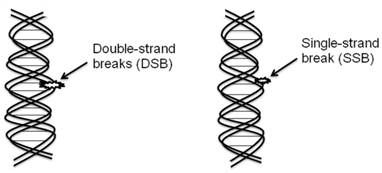
Figure 1. Direct and Indirect DNA Damage Induced by Ionizing Radiation [1]
Schematic representation: A cell containing a nucleus with DNA is depicted.
Two principal mechanisms of radiation-induced damage are illustrated:
- Direct effect — the radiation track intersects the DNA molecule, causing strand breaks.
- Indirect effect — radiolysis of water leads to the formation of free radicals, which subsequently damage DNA bases and strands, resulting in the formation of double-strand breaks (DSBs).
Double-strand breaks (DSBs) are highlighted as the key lethal form of radiation-induced DNA damage.
Conceptually, the evolution of radiation therapy technologies (3D-CRT → IMRT/VMAT → IGRT → SBRT/SRS → proton/ion therapy and adaptive approaches) reflects the effort to “sculpt” the dose distribution around the spinal cord while preserving therapeutic efficacy within tumor tissue. The fundamental principles of modern techniques—namely inverse planning, beam intensity modulation, and enhanced geometric precision through image guidance—are comprehensively described in reviews on radiation physics and radiobiology [1, 6].
From a clinical standpoint, spinal metastases represent a model scenario in which the “cost” of technological advantage becomes particularly evident. Randomized trials evaluating analgesic outcomes have demonstrated heterogeneous results. In the phase II/III SC.24 trial, SBRT delivered as 24 Gy in 2 fractions achieved a higher complete pain response rate at 3 months compared with 20 Gy in 5 fractions in a carefully selected patient cohort (limited number of treated segments, controlled mechanical stability according to SINS, and absence of symptomatic spinal cord compression) [9]. Conversely, in the phase III NRG/RTOG 0631 study, comparison of SRS/SBRT (16–18 Gy in 1 fraction) with conventional radiation therapy (8 Gy in 1 fraction) did not demonstrate superiority of SRS in the primary endpoint—patient-reported pain response at 3 months. Importantly, no severe spinal cord toxicity was observed during 24 months of follow-up [10]. The practical conclusion from these data must be formulated cautiously: SBRT/SRS for spinal metastases demonstrates substantial potential, but its advantage depends on study design, comparator regimen (20 Gy/5 fractions versus 8 Gy/1 fraction), inclusion criteria (mechanical stability, epidural extension, radioresistant histology), and quality of treatment delivery (IGRT, planning quality assurance, multidisciplinary expertise). Consequently, clinical guidelines—including national recommendations—may adopt a restrained position regarding routine SBRT use in vertebral metastases, particularly in the presence of spinal cord compression [2].
An additional major domain is the treatment of metastatic epidural spinal cord compression (MESCC). Here, the balance between decompression and dose safety is implemented through a “hybrid strategy”: separation surgery to create a minimal safe margin between tumor and spinal cord, followed by SBRT. A prospective single-center phase II study demonstrated that separation surgery combined with SBRT (24 Gy in 2 fractions) achieved effective decompression (reduction to Bilsky grade ≤1 in most patients) and acceptable 12-month local control. Reported complications included vertebral compression fractures [11]. A recognized toxicity of spinal SBRT is the risk of vertebral compression fractures (VCF). Systematic analyses indicate that the estimated incidence of VCF after SBRT ranges from approximately 11% to 39%, significantly higher than after conventional RT (around 5%). The risk is influenced by baseline bone destruction, anatomical location, tumor volume, and dose parameters [12].
Risk stratification tools are essential in treatment planning. The Spinal Instability Neoplastic Score (SINS) standardizes assessment of neoplastic spinal instability based on clinical and radiographic criteria and guides the need for surgical consultation or stabilization procedures. In the SC.24 trial, SINS restrictions were incorporated as part of patient selection criteria [13]. In primary spinal tumors such as chordomas, proton and ion therapy play a significant role due to the requirement for dose escalation with maximal spinal cord sparing. A retrospective proton therapy series (58 patients) demonstrated high local control rates at a median dose of approximately 70 CGE with acceptable late toxicity; tumor location (e.g., cervical spine) was associated with inferior local control in some cases. A national multicenter study of carbon-ion therapy for sacral chordomas (219 patients) reported 5-year local control of approximately 72% using a commonly applied regimen of 67.2 Gy (RBE) in 16 fractions, with relatively low rates of severe toxicity [14]. In bone marrow tumors in the narrow sense (plasmacytomas, multiple myeloma), radiation therapy most often serves a palliative and organ-preserving function—pain control, treatment of compression, and prevention of pathological fractures. In contrast, for solitary plasmacytoma of the spine, local RT remains the standard of care with curative intent. Reviews emphasize the use of moderate total doses (approximately 40–50 Gy with conventional fractionation), with mandatory consideration of MRI findings and proximity to critical structures [15].
A further important intersection between radiation oncology and transplantation medicine is represented by total marrow irradiation (TMI) and total marrow and lymphoid irradiation (TMLI). Unlike traditional total body irradiation (TBI), TMLI enables selective irradiation of bone marrow and lymphoid structures while reducing dose exposure to organs at risk. Contemporary reviews consider TMI/TMLI as a more targeted evolution of radiation-based conditioning. Clinical studies (e.g., TMLI 2000 cGy delivered as 200 cGy twice daily) demonstrate potential reduction in severe toxicity while maintaining acceptable survival outcomes in selected cohorts, although these approaches remain highly specialized and resource-intensive [16].
Table 1.
Clinical Studies of Contemporary Radiation Therapy Techniques for Spinal and Bone Marrow Tumors
|
Study |
Year |
Design / Population |
n |
Regimen / Technology |
Main Outcomes (Local Control / Pain / Toxicity) |
|
Sahgal A. et al., SC.24 |
2021 |
Randomized phase II/III; painful spinal metastases; strict selection (≤3 segments, SINS <12, no symptomatic cord compression) |
229 |
SBRT 24 Gy / 2 fractions vs cEBRT 20 Gy / 5 fractions |
Complete pain response at 3 months: 35% vs 14%; severe adverse events rare; no treatment-related deaths. |
|
Ryu S. et al., NRG/RTOG 0631 |
2023 |
Randomized phase II/III; 1–3 vertebral metastases |
339 |
SRS/SBRT 16–18 Gy / 1 fraction vs cEBRT 8 Gy / 1 fraction |
No superiority of SRS for 3-month pain response; no radiation myelopathy over 24 months; VCF ≈20% in both groups. |
|
Ito K. et al. |
2022 |
Prospective phase II; symptomatic MESCC; separation surgery + RT |
33 |
Separation surgery + SBRT 24 Gy / 2 fractions |
12-month local failure 13%; significant reduction in Bilsky grade; VCF observed in some patients; no clinically significant myelopathy. |
|
Sahgal A. et al. (VCF analysis) |
2013 |
Analytical review / pooled data on VCF after spinal SBRT |
— |
Spinal SBRT |
Estimated VCF risk higher after SBRT than conventional RT; reported range ~11–39% vs ~5% (conventional). |
|
Youn S.H. et al. |
2018 |
Retrospective series; chordomas (spine/sacrum) |
58 |
Proton therapy; median dose 69.6 CGE |
5-year LPFS ~88%, OS ~88%; ≥G3 late toxicity rare; tumor location influenced failure pattern. |
|
Demizu Y. et al. |
2021 |
Retrospective multicenter (Japan); sacral chordomas |
219 |
Carbon-ion RT; commonly 67.2 Gy (RBE) / 16 fractions |
5-year local control ~72%; ≥G3 acute toxicity ~4%; late ≥G3 ~6%. |
|
Stein A.S. et al. |
2022 |
Prospective study; AML in remission; conditioning before allo-HCT |
18 |
TMLI 2000 cGy (200 cGy twice daily); organ-sparing approach |
No Bearman grade 3–4 toxicity or treatment-related mortality; low GVHD incidence; 2-year OS ~87%; NRM 0% (small cohort). |
Practical Recommendations and Limitations
Clinical decision-making in spinal tumors almost always begins with identification of the currently dominant factor: pain syndrome, neurological deficit/spinal cord compression, mechanical instability, or overall systemic prognosis. The NOMS framework emphasizes a multidisciplinary approach and links the choice of radiation therapy to the extent of epidural disease and tumor radiosensitivity. In practice, this implies the following: in cases of high risk or clinically significant spinal cord compression, surgical decompression and/or stabilization should be considered; in stable patients without compression, the choice lies between palliative regimens and SBRT depending on therapeutic priorities (rapid pain relief versus durable local control) [3]. For symptomatic bone metastases (including spinal involvement), Russian clinical guidelines allow single-fraction irradiation of 8 Gy in patients with limited mobility and unfavorable prognosis, as well as fractionated regimens (e.g., 24 Gy/6 fractions, 25 Gy/5, 30 Gy/10) in patients with better performance status. A high rate of analgesic response is emphasized, along with the need to inform patients about the possibility of re-irradiation after single-fraction treatment. These regimens are consistent with international recommendations (ESTRO/ACROP), which also provide schedules for spinal cord compression in non-operable patients (8 Gy/1, 16 Gy/2, 20 Gy/5, 30 Gy/10) [2].
The use of SBRT for spinal lesions requires adherence to three fundamental constraints. First, strict patient selection (mechanical stability, limited disease extent, absence of uncontrolled epidural involvement). Second, prioritization of spinal cord safety using contemporary dose constraints (HyTEC) and appropriate accounting for cumulative dose in re-irradiation, including conversion to equivalent dose in 2 Gy fractions (EQD2) and respect of adequate intervals between treatment courses. Third, assessment of vertebral compression fracture (VCF) risk: in cases of pronounced lytic destruction or instability, prophylactic stabilization should be considered and extreme dose escalation avoided [7].
Re-irradiation of the spine represents a particularly high-risk scenario. HyTEC recommendations indicate that repeat SBRT may be feasible under strict cumulative dose control to the thecal sac and spinal cord, justified fractionation selection, and sufficient inter-treatment interval. Practical implementation requires standardized contouring and mandatory dose conversion into EQD2 to ensure comparability with prior courses [8]. In bone marrow tumors (multiple myeloma, plasmacytomas), preservation of functional bone marrow reserve for subsequent systemic therapy remains the principal limitation. Russian guidelines emphasize that escalation of total dose to 30–50 Gy does not improve outcomes but increases the risk of prolonged myelosuppression. Contemporary literature supports the concept of “low but effective doses” in palliative settings—achieving symptom control without compromising further systemic treatment. In solitary spinal plasmacytoma, however, the strategy differs: local RT is delivered with moderately radical doses of approximately 40–50 Gy in standard fractionation, with mandatory MRI-based planning and careful consideration of adjacent critical structures [8]. Recent innovative directions—adaptive radiation therapy (ART), artificial intelligence-assisted contouring and planning, FLASH irradiation, and further development of proton and ion therapy—show significant potential. However, in spinal and bone marrow tumors, these technologies currently complement rather than replace established evidence-based practice. The most realistic near-term contribution lies in further reduction of delivery uncertainties, optimization of SBRT/ART workflows, and more individualized complication risk assessment (radiation myelopathy, VCF, myelosuppression) [4].
Conclusion
Radiation therapy for spinal and bone marrow tumors represents a field in which physical dose-distribution principles, radiobiological damage mechanisms, and clinical treatment strategy converge within millimeter-scale tolerances. The quality of imaging, planning precision, and strict adherence to dose constraints determine the feasibility of delivering a therapeutically effective tumor dose while preventing irreversible spinal cord injury and critical suppression of bone marrow hematopoiesis. Conventional palliative radiation therapy remains the foundation of treatment for pain and skeletal-related complications in metastatic disease. Stereotactic techniques, as well as proton and ion therapy, expand the potential for local control but require strict patient selection, rigorous dose constraints, and high technical execution standards. In cases of epidural spinal cord compression, hybrid strategies combining surgical decompression with high-precision irradiation play a critical role. The inconsistency of randomized data regarding pain response in spinal metastases underscores the need for precise patient selection, harmonization of efficacy assessment criteria, and standardization of study endpoints. These factors largely explain discrepancies between international and certain national clinical guidelines and highlight the ongoing need for further research aimed at optimizing the therapeutic index in spinal and bone marrow involvement.
Список литературы
- Laufer I, Rubin DG, Lis E, et al. The NOMS framework: approach to the treatment of spinal metastatic tumors. The Oncologist. 2013;18(6):744–751. doi:10.1634/theoncologist.2012-0293
- Association of Oncologists of Russia. Metastatic bone disease in malignant neoplasms: clinical guidelines. 2023. Available at: https://oncology-association.ru/wp-content/uploads/2023/06/metastaticheskoe-porazhenie-kostej-pri-zlokachestvennyh-novoobrazovaniyah.pdf (accessed February 26, 2026)
- Ryu S, Deshmukh S, Timmerman RD, et al. Stereotactic radiosurgery vs conventional radiotherapy for localized vertebral metastases of the spine: Phase 3 results of NRG Oncology/RTOG 0631 randomized clinical trial. JAMA Oncology. 2023. doi:10.1001/jamaoncol.2023.0356
- Sahgal A, Myrehaug SD, Siva S, et al. Stereotactic body radiotherapy versus conventional external beam radiotherapy in patients with painful spinal metastases: an open-label, multicentre, randomised, controlled, phase 2/3 trial. The Lancet Oncology. 2021. doi:10.1016/S1470-2045(21)00196-0
- Kirkpatrick JP, van der Kogel AJ, Schultheiss TE. Radiation dose–volume effects in the spinal cord. International Journal of Radiation Oncology Biology Physics. 2010;76(Suppl 3):S42–S49. doi:10.1016/j.ijrobp.2009.04.095
- Sahgal A, Chang JH, Ma L, et al. Spinal cord dose tolerance to stereotactic body radiation therapy. International Journal of Radiation Oncology Biology Physics. 2021;110(1):124–136. doi:10.1016/j.ijrobp.2019.09.038
- Fisher CG, DiPaola CP, Ryken TC, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine. 2010;35(22):E1221–E1229. doi:10.1097/BRS.0b013e3181e16ae2
- Guckenberger M, et al. ESTRO clinical practice guideline: stereotactic body radiotherapy for spine metastases. Radiotherapy and Oncology. 2024;190:109966. doi:10.1016/j.radonc.2023.109966
- Oldenburger E, et al. ESTRO ACROP guidelines for external beam radiotherapy of patients with complicated bone metastases. Radiotherapy and Oncology. 2022. doi:10.1016/S0167-8140(22)04147-0
- Clinical guidelines: Multiple myeloma. 2014. Available at: https://blood.ru/documents/clinical%20guidelines/20.%20klinicheskie-rekomendacii-2014-mieloma.pdf (accessed February 26, 2026)
- Elhammali A, Amini B, Ludmir EB, et al. New paradigm for radiation in multiple myeloma: lower yet effective dose to avoid radiation toxicity. Haematologica. 2020;105(7):e355–e357. doi:10.3324/haematol.2019.235804
- Koçak E, et al. Solitary plasmacytoma. Turkish Journal of Hematology. 2010;27:57–61
- Ito K, Sugita S, Nakajima Y, et al. Phase 2 clinical trial of separation surgery followed by stereotactic body radiation therapy for metastatic epidural spinal cord compression. International Journal of Radiation Oncology Biology Physics. 2022;112(1):106–113. doi:10.1016/j.ijrobp.2021.07.1690
- Sahgal A, Atenafu EG, Chao S, et al. Vertebral compression fracture after spine stereotactic body radiotherapy: a multi-institutional analysis. Journal of Clinical Oncology. 2013. doi:10.1200/JCO.2013.50.1411
- Sahgal A, et al. Vertebral compression fracture after stereotactic body radiotherapy for spinal metastases. The Lancet Oncology. 2013;14(8):e310–e320. doi:10.1016/S1470-2045(13)70101-3
- Youn SH, Cho KH, Kim JY, et al. Clinical outcome of proton therapy for patients with chordomas. Radiation Oncology Journal. 2018;36(3):182–191. doi:10.3857/roj.2018.00164
- Demizu Y, Imai R, Kiyohara H, et al. Carbon ion radiotherapy for sacral chordoma: a retrospective nationwide multicentre study in Japan. Radiotherapy and Oncology. 2021;154:1–5. doi:10.1016/j.radonc.2020.09.018
- Stein AS, Al Malki MM, et al. Total marrow and lymphoid irradiation with post-transplant cyclophosphamide for patients with AML in remission. Transplantation and Cellular Therapy. 2022
- Wong JYC, Filippi AR, Scorsetti M, et al. Total marrow and total lymphoid irradiation in bone marrow transplantation for acute leukaemia. The Lancet Oncology. 2020;21(10):e477–e487. doi:10.1016/S1470-2045(20)30342-9
- Baskar R, Lee KA, Yeo R, Yeoh KW. Cancer and radiation therapy: current advances and future directions. International Journal of Medical Sciences. 2012;9(3):193–199. doi:10.7150/ijms.3635
- Mehta SR, Suhag V, Semwal M, Sharma N. Radiotherapy: basic concepts and recent advances. Medical Journal Armed Forces India. 2010;66(2):158–162. doi:10.1016/S0377-1237(10)80132-7
- Webster M, Podgorsak A, Li F, et al. New approaches in radiotherapy. Cancers. 2025;17(12):1980. doi:10.3390/cancers17121980



